Tricuspid Valve
Tricuspid regurgitation can be treated by replacing the native valve (TTVR) or by repairing the native valve (TTVr). Planning for both types of procedures can be done using the 3mensio Tricuspid Valve workflow.
Request a demoTricuspid Valve Anatomy & Function
Where is the Tricuspid Valve Located?
The tricuspid valve is one of the four valves of the human heart, located between the right atrium and the right ventricle. The function of the tricuspid valve is to ensure that blood flows in the correct direction, from the atrium into the ventricle, and to prevent blood from leaking backward when the ventricle contracts. When the right atrium contracts, the valve opens, allowing blood to move into the right ventricle. When the ventricle contracts, the valve closes tightly to stop blood from flowing back into the atrium. This one-way system maintains efficient circulation.
Anatomy of the Tricuspid Valve
The valve has three leaflets (or cusps): anterior, posterior, and septal. These thin but strong flaps of tissue open and close with each heartbeat. They are supported by:
- Chordae tendineae (string-like structures) that connect the leaflets to the papillary muscles.
- Papillary muscles within the right ventricle that contract to stabilize the valve during the heartbeat.
- Annulus (the fibrous ring) that forms the structural base of the valve and maintains its shape.
Together, these components ensure a one-way flow of blood toward the lungs for oxygenation. Why tricuspid valve function matters is because of the following reason. Although it receives less attention than the mitral or aortic valves, the tricuspid valve plays a vital role in right heart function. Abnormalities can result in conditions such as tricuspid regurgitation (leakage) or tricuspid atresia (congenital absence of the valve), which may cause fatigue, swelling, and heart rhythm disturbances.
What Is Tricuspid Regurgitation?
Tricuspid regurgitation (TR) occurs when the tricuspid valve does not close tightly. As a result, blood leaks backwards into the right atrium each time the right ventricle contracts. Many people are surprised to learn that mild or even trivial tricuspid regurgitation is a very common finding on echocardiograms. In most cases, this does not cause problems and is considered a normal variation. However, in some patients, tricuspid regurgitation progresses from mild to moderate or even severe, which can significantly affect heart function.
Causes of Tricuspid Regurgitation
The condition may develop in different ways:
- Primary TR occurs when the valve itself is abnormal, due to congenital malformations, rheumatic disease, or injury from infection or devices such as pacemaker leads.
- Secondary or Functional TR is more common and happens when the right side of the heart enlarges due to conditions such as pulmonary hypertension, left-sided valve disease, or atrial fibrillation. The valve leaflets are structurally normal, but the stretching of the valve ring prevents them from sealing properly.
In many people, especially when mild, TR is detected incidentally on echocardiography and does not cause symptoms.
How Imaging Is Used to Diagnose of Tricuspid Regurgitation
Tricuspid regurgitation is often suspected during a physical examination when a physician hears a systolic murmur along the lower left sternal border or observes signs of right-sided heart failure such as jugular venous distention, ascites, or leg swelling.
The gold standard for diagnosis is echocardiography. Transthoracic echocardiography (TTE) is usually the first test, providing information on leaflet anatomy, regurgitant jet direction, and chamber dimensions. Doppler echocardiography is particularly valuable for quantifying regurgitant flow and grading severity. Transesophageal echocardiography (TEE) may be performed when higher-resolution imaging is required, especially before an intervention.
In selected cases, advanced imaging may be used. Cardiac MRI provides highly accurate assessment of right ventricular size and function, while cardiac CT can help define annular dimensions and surrounding structures when planning surgical or transcatheter therapies. Additional tests such as electrocardiography (ECG) and chest X-ray may reveal rhythm disturbances or right atrial enlargement but are not diagnostic on their own.
By combining clinical examination with multimodality imaging, cardiologists can accurately grade tricuspid regurgitation and determine the best timing for follow-up or intervention.
Types and Severity of TR
Trivial and Mild TR
Trivial or mild tricuspid regurgitation is very common and usually has no clinical impact. It is often described as a normal variation of blood flow across the tricuspid valve. In these cases, there are no symptoms, and no treatment is required apart from routine check-ups.
Moderate TR
When regurgitation becomes moderate, some patients may notice fatigue, mild swelling of the ankles, or irregular heartbeats. Regular follow-up is important at this stage because the condition can progress over time. Doctors usually recommend repeat echocardiograms every one to two years to monitor changes.
Severe TR or Torrential TR
Severe leakage significantly impairs heart function. Patients may develop leg swelling, abdominal bloating, liver congestion, and pronounced neck vein pulsations. In torrential TR, the backward flow of blood is extreme and often requires surgical or transcatheter valve repair or replacement.
Symptoms and Early Warning Signs
While mild regurgitation often remains silent, even mild cases should be followed up, as the condition can progress. If symptoms appear, it is usually a sign that the regurgitation has moved beyond a trivial or mild stage, which is why regular follow-up imaging is key.
Tricuspid Regurgitation in Special Conditions
Functional TR and Associated Diseases
In many patients, TR develops not because the valve is abnormal, but because the heart is enlarged. This type, called functional tricuspid regurgitation, is frequently associated with pulmonary hypertension, long-standing atrial fibrillation, or left-sided heart conditions such as mitral valve disease.
When TR occurs together with other valve diseases — for example, mitral regurgitation (MR) and tricuspid regurgitation (TR) — the risk of heart failure increases significantly. In these cases, doctors often consider treating both valves at the same time, either with surgical repair or minimally invasive catheter-based therapies.
Rare and Unique Presentations
In some cases, TR may be related to congenital abnormalities such as Ebstein’s anomaly. It can also occur after device implantation, when pacemaker or ICD leads interfere with the valve’s normal function (CIED-related Cardiac implantable electronic device). Echocardiography sometimes reveals findings like “V wave TR”, which signal significant backflow and usually correlate with advanced disease.
Living With and Monitoring TR
For most people with mild or trivial TR, no treatment is necessary. Moderate TR typically requires regular checkups and management of underlying conditions such as high blood pressure or atrial fibrillation. Severe and torrential TR may require intervention, which can include valve repair or replacement.
In summary, tricuspid regurgitation is a spectrum ranging from trivial findings of no clinical concern to severe and torrential disease that requires surgical or interventional therapy. Mild and moderate TR often remain stable for years, but progression is possible, particularly in patients with associated heart disease. Special conditions such as, pulmonary hypertension, and combined valve disease require tailored management.
Understanding the severity, monitoring symptoms, and maintaining regular follow-up with a cardiologist are essential steps in ensuring the best possible outcomes for patients with tricuspid regurgitation.
How to treat tricuspid regurgitation?
How to treat any type of TR is best described in the flow chart below. The most common treatment strategies are Tricuspid Repair (like annuloplasty or T-TEER transcather edge to edge repair) or Tricuspid Replacement (surgical replacement or TTVR, Transcather Tricuspid Valve Replacement).
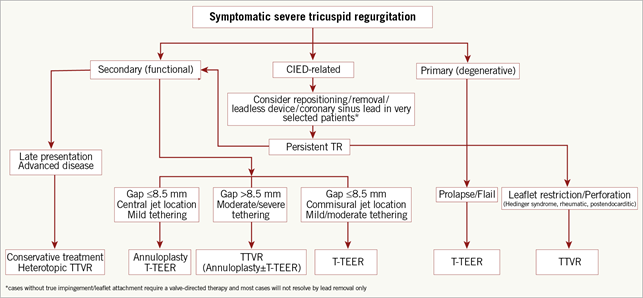
From: Praz, F., Muraru, D., Kreidel, F., Lurz, P., Hahn, R. T., Delgado, V., Senni, M., von Bardeleben, R. S., Nickenig, G., Hausleiter, J., Mangieri, A., Zamorano, J. L., Prendergast, B. D., & Maisano, F. (2021, November 19). Transcatheter treatment for tricuspid valve disease. EuroIntervention, 17(10), 791–808. https://doi.org/10.4244/EIJ-D-21-00695
Tricuspid Valve Repair
Tricuspid valve repair is a surgical or transcatheter (TTVr) approach to correct malfunctioning valve tissue without replacing it. It is often preferred over replacement because it:
- Preserves the native valve structure
- Reduces the need for long-term anticoagulation therapy
- Leads to better long-term outcomes in select patients
Surgical repair options include:
- Annuloplasty rings to tighten the valve opening
- Leaflet reconstruction to address torn or prolapsed leaflets
- Chordae re-suspension to restore normal motion of the valve
This approach is often recommended for moderate to severe tricuspid regurgitation or combined mitral and tricuspid disease, especially when caught early.
Diagnosis and Imaging for Tricuspid Valve Repair
Accurate diagnosis and planning are critical for successful valve repair. Imaging techniques include:
- Echocardiography (TTE/TEE): First-line imaging to assess valve anatomy and function.
- Cardiac CT: Essential in preoperative planning and device sizing.
- CT allows:
- High-resolution visualization of the tricuspid annulus
- Measurement of right atrial and ventricular volumes
- Evaluation of surrounding structures like the right coronary artery
- Assessment of annular calcification or leaflet morphology
Devices Used for Transcatheter Tricuspid Valve Repair (TTVr)
Several technologies have emerged to address tricuspid valve dysfunction, especially in patients who are not surgical candidates:
- Annuloplasty Devices: Like the Cardioband, these reshape or cinch the valve annulus.
- Leaflet Grasping Devices (TEER, Transcatheter Edge to Edge Repair) devices: Devices such as TriClip™ or PASCAL help clip together leaky leaflets.
- Spacer Devices: Devices such as FORMA, positioned in the center of the valve to reduce regurgitation gap.
Each device is selected based on valve anatomy, severity of regurgitation, and overall cardiac function.
Health Risks and Complications with Tricuspid Valve Repair
While tricuspid valve repair is less invasive than replacement and offers excellent outcomes in many patients, it is not without risk. Potential complications include:
- Bleeding or infection
- Residual regurgitation or stenosis
- Conduction abnormalities (e.g., heart block)
- Device malposition in transcatheter approaches
- Need for future valve replacement if repair fails
Tricuspid valve repair offers a valuable treatment pathway for restoring right heart function while preserving natural anatomy. Early diagnosis and comprehensive imaging, including cardiac CT, are critical to achieving optimal outcomes. However, when the regurgitation gap is too big for repair, tricuspid valve replacement becomes necessary. Replacement involves using either transcatheter or bioprosthetic valves and may carry higher long-term risks and complications.
The Role of Tricuspid Valve Replacement
Tricuspid valve replacement is performed when the valve is too damaged to be repaired, or if prior repair has failed. Unlike repair, this procedure involves removing the native valve and implanting a new one, either through open-heart surgery or transcatheter techniques.
It is typically indicated in cases of:
- Severe regurgitation or stenosis not responsive to medical management or repair
- Valve endocarditis or calcification
- Congenital malformations incompatible with repair
- Structural deterioration of a previously repaired or replaced valve
In this procedure, the damaged valve is removed and replaced with an artificial valve, which can be either mechanical, biological (tissue-based), or transcatheter TTVR (Transcatheter Tricuspid Valve Replacement).
In some patients who have undergone a prior annuloplasty, a “valve-in-ring” (ViR) procedure may be performed, where a new transcatheter valve is implanted inside the existing surgical ring to restore function without the need for reoperation.
Imaging Techniques for Tricuspid Valve Replacement
Pre-procedural imaging is critical to guide valve sizing, approach planning, and procedural safety.
- Echocardiography (TTE/TEE): Used for initial assessment of valve function and anatomy.
- Cardiac CT: Plays a major role in replacement planning, especially for transcatheter tricuspid valve replacement (TTVR). CT helps with:
- Detailed 3D mapping of the tricuspid annulus
- IVC – Annulus offset measurement
- Measurement of landing zone and annular dimensions
- Visualization of proximity to critical structures such as the right coronary artery
- Identifying calcifications or anomalies that may affect anchoring of the prosthesis
Devices Used for Tricuspid Valve Replacement
Tricuspid valve replacement can involve:
- Mechanical Valves: Mechanical valves are made from metal or carbon materials and are often surrounded by a polyester fabric ring for improved integration with the heart tissue. These valves are highly durable and can last a lifetime, but they require lifelong use of blood-thinning medication (anticoagulants) to prevent blood clots and stroke.
- Surgical Bioprosthetic Valves: Tissue valves are made from pig or cow heart tissue and tend to mimic natural valve movement more closely. While they typically last 10 to 15 years, they generally do not require lifelong anticoagulation, making them ideal for older patients or those with contraindications to blood thinners.
- Transcatheter Devices (TTVR): Transcatheter Tricuspid Valves: Several transcatheter valve replacement systems have been developed to treat severe tricuspid regurgitation in patients at high surgical risk. Most transcatheter tricuspid valves, such as the EVOQUE, LuX-Valve, NaviGate, Intrepid, and V-Dyne, are designed for orthotopic replacement of the native tricuspid valve, anchoring within the annulus to restore leaflet function. In contrast, the TricValve system is implanted in the vena cavae rather than the valve itself, aiming to reduce venous backflow and relieve symptoms without replacing the tricuspid valve.
These emerging technologies offer a minimally invasive alternative for high-risk or inoperable patients.
Health Risks and Complications with Tricuspid Valve Replacement
While valve replacement can be life-saving, it comes with risks such as:
- Bleeding, stroke, or infection
- Valve thrombosis or degenerations
- Conduction system damage (e.g., need for pacemaker)
- Lifelong anticoagulation for mechanical valves
- Device migration or paravalvular leak in transcatheter procedures
Importantly, replacement is often the last resort when repair is no longer feasible or has failed. The choice between repair and replacement depends on type of regurgitation, valve condition, patient age, comorbidities, and anatomical complexity.
Tricuspid valve replacement is a vital option for patients with advanced valve disease, restoring heart function and alleviating severe symptoms when repair is not feasible.
Advanced imaging—particularly cardiac CT—plays a central role in ensuring safety and effectiveness, guiding both surgical and transcatheter approaches. By integrating 3mensio Structural Heart with CT, clinicians gain precise support for device placement during transcatheter tricuspid repair as well as comprehensive planning for valve replacement, assisting with tailored treatment strategies.